By Hayley Iosue, DPM, Joseph Albright, DPM, and Mark Mendeszoon, DPM
By Hayley Iosue, DPM, Joseph Albright, DPM, and Mark Mendeszoon, DPM
Chronic compartment syndrome is an often-overlooked diagnosis in patients who are athletically inclined. With an average 22-month delay in diagnosis, suspicions need to be elevated sooner.
Leg pain in the active and athletic patient population can be difficult to evaluate, diagnose, and treat. A physician must be aware of many causes of lower extremity pain in these patients. Lower leg pain experienced by athletes is typically posterior tibial tendonitis, shin splints, stress fractures, or Achilles tendonosis. Exertional chronic compartment syndrome is not a common diagnosis; however, it is one that is commonly overlooked. There is typically a 22-month delay in the diagnosis and treatment of chronic compartment syndrome and popliteal artery entrapment in patients, and that delay could be detrimental to their athletic career.1
Chronic compartment syndrome is caused by increased pressure within the closed fibro-
osseous spaces and the anatomic compartments. It is thought to lead to reduced blood flow and tissue perfusion and is associated with repetitive exertion. While it is most commonly seen in the lower leg, it has been described in the shoulder, arms, hands, thighs, and feet. Incidence ranges from 14% to 39% in the general population presenting with leg pain.2 Typically, this condition is seen in athletics that require running and jumping thus leading to increased intramuscular pressure during training or competition.
Acute compartment syndrome, which is often seen in fractures or crush injuries to the extremities, represent emergencies and are outside the scope of this article.
Anatomy Is Key
 It is imperative to understand the anatomy in the evaluation, diagnosis, and treatment of chronic compartment syndrome. Historically, the lower leg has been described as four compartments. Each compartment contains individual muscles, nerves, arteries, and veins, encased in its own fascial membrane.
It is imperative to understand the anatomy in the evaluation, diagnosis, and treatment of chronic compartment syndrome. Historically, the lower leg has been described as four compartments. Each compartment contains individual muscles, nerves, arteries, and veins, encased in its own fascial membrane.
- The anterior compartment contains the anterior tibial artery, deep peroneal nerve, extensor digitorum longus, anterior tibialis, and extensor halluces longus.
- The lateral compartment encloses the superficial peroneal nerve and the peroneus longus and brevis muscles.
- The superficial posterior compartment contains the sural nerve, the medial and lateral heads of the gastrocnemius muscles, and the soleus muscle.
- The deep posterior compartment contains the tibial nerve, posterior tibial artery, peroneal artery, the flexor digitorum brevis, and the flexor hallucis brevis.
- A more recent theory is that there is a fifth compartment which is made up only of the posterior tibialis muscle with its own fascial covering.3
Chronic compartment syndrome most commonly involves the anterior and lateral compartments.4
During repetitive and strenuous exercise, muscle fibers can swell up to 20 times their resting size. This is due to increased blood flow and edema, which can cause a 20% increase in muscle volume and weight.5 A normal compartment is able to accommodate such physiological changes during exercise; however, a non-compliant compartment will lead to increased intra-compartmental pressures. In a non-compliant compartment, the increased perfusing blood volume, muscle hypertrophy, and increased interstitial fluid volume will allow increased pressure in accordance with Laplace’s law. This law explains that a capillary membrane subjected to internal and external pressures reaches an equilibrium based on those forces. This equilibrium will cause a decrease in both arteriolar flow and venous return. In non-compliant compartments, it is thought that blood flow becomes insufficient to meet the requirements of the muscle, thus creating pain with activity.6
The pain was originally thought to be an ischemic pain related to the decreased oxygenation of the tissues, insufficient muscle perfusion, and decreased return. However, some studies have found that this may not be the case. Amendola et al 7 used nuclear medicine blood flow studies to evaluate alterations in the muscles during chronic compartment syndrome, and saw no ischemic changes in the muscles. Balduini et al8 used P-NMR spectroscopy to evaluate for ischemic changes in the muscle. They found that ischemic changes only occurred at very high pressures (>160mmHg) which are typically not seen in exertional compartment syndrome. Another theory is the pain is related to the stimulation of the fascia or the periosteal sensory nerves related to the increased pressure within the compartment. The local release of kinins along with reduced blood flow could also be another source of the pain.9

The Physical Exam
A thorough history and physical exam is crucial to the diagnosis of compartment syndrome. The trick is to watch these patients exercise first and examine them immediately afterward.
The patient will describe a history of pain with chronic exertion. Athletes typically performing a repetitive exercise describe a dull ache that begins around the same time or distance during their exercise; the pain worsens to the point that they must stop. This pain will be relieved by rest. The patient also may describe a tightness or stiffness in their legs. In more advanced cases, patients can also experience transient numbness, tingling or drop foot. At rest, a patient’s physical exam is normal: the patient will have no signs or symptoms at rest. In about 40% to 60% of patients, fascial herniation is present during an at-rest exam.10 However, after these patients exercise, the exam has more significant findings: The compartments will appear tense, firm, and occasionally, the skin will appear shiny. The patient may have weakness or decreased sensation in the foot.
The differential diagnosis for leg pain includes, but is not limited to, stress fractures, stress reactions, bone tumors, complex regional pain syndrome, radiculopathy, and popliteal artery entrapment syndrome.
Imaging may be useful in the diagnosis of chronic compartment syndrome but it is not the mainstay of diagnosis. Plain radiographs can be useful to help rule out stress fractures, reactions, or other boney abnormalities. An MRI can be utilized to see if there is any structural or soft tissue anomaly that may compress the popliteal artery. Bone scans have been utilized to show an ischemic compartment if needed. The gold standard test for diagnosing compartment syndrome is compartment pressure testing at rest and with exercise.
Compartment pressure measurements can be done with a wick catheter, slit catheter, mircotip, microcapillary infusion, or a needle manometer. Measurements should be taken at rest, and then within 1 minute of exercise and then at 5 minutes post-exercise. The patient should be lying in a comfortable position with the foot plantarflexed at 20 degrees and the knee in 10 to 30 degrees of flexion. Measuring the compartment pressures can be difficult so it is important to be familiar with the anatomy and equipment being used for measurements. Pedowitz et al11 defined a set of criteria to diagnose chronic compartment syndrome. At least 1 of the following 3 criterion has to be present: a resting pressure greater than or equal to 115mmHg, a measurement taken 1 minute post-exercise greater than 30mmHg, or a measurement taken 5 minutes post-exercise greater than 20mmHg.
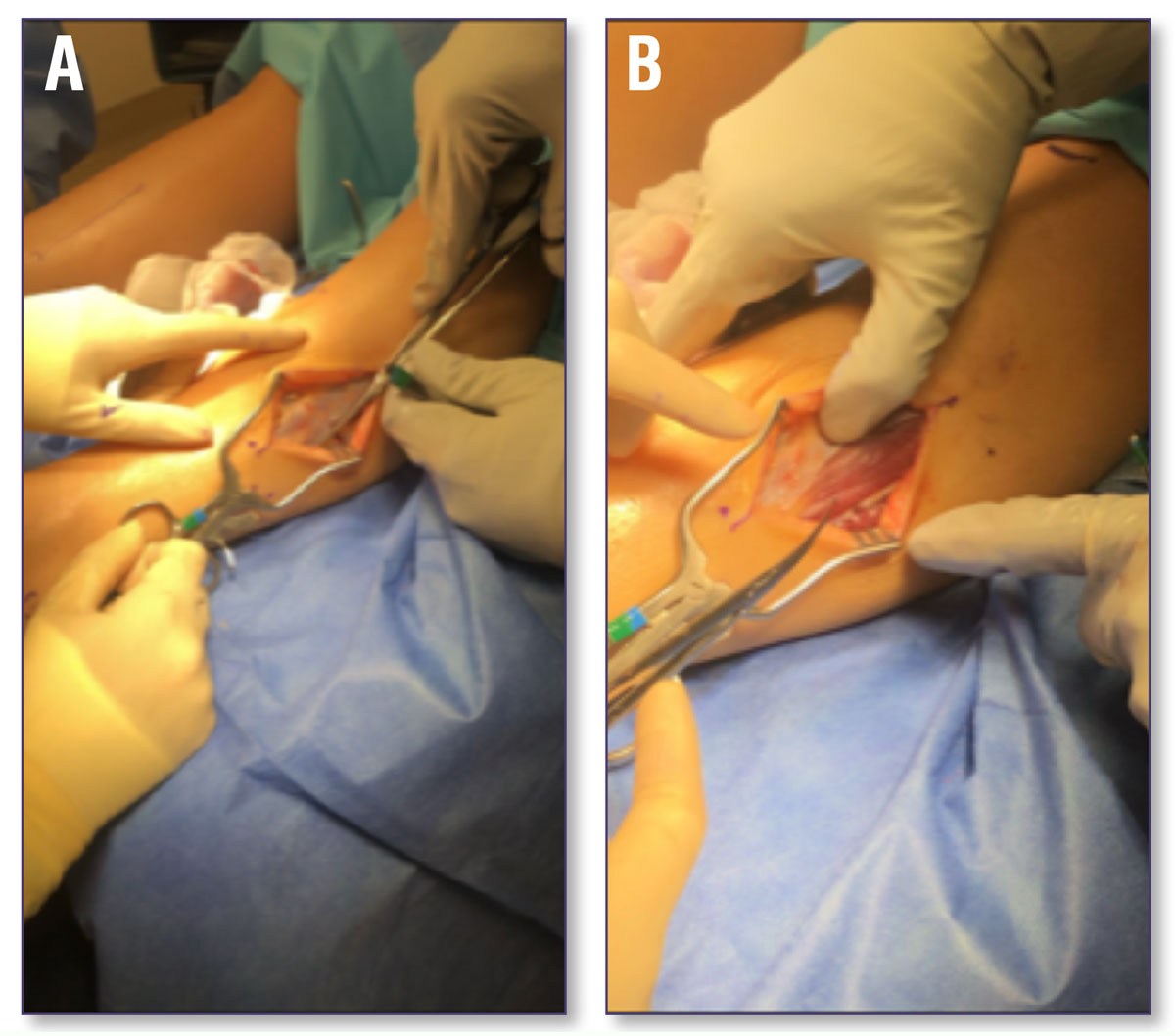
Figure 2. Surgical approach to anterior lateral compartment release: A) before fascial release; B) post-surgical release. Photos provided by the authors.
Treatment Options
After a diagnosis of chronic exertional compartment syndrome is made, treatment options will need to be discussed with the patient. Few conservative treatment options are typically amenable to these patients. The patient can stop the activity which aggravates the symptoms; however, many patients are not agreeable with this option. The patient can try rest, NSAIDs, and/or ice to help alleviate the symptoms. Blackman et al12 found that massage therapy was helpful in 7 patients in a retrospective cohort study. After a 5-week massage and stretching program, the patients were able to increase the amount of work performed during exercise before the symptoms developed.
Many of these patients will elect to undergo surgical intervention with fasciotomies of the affected compartments. The fasciotomies can be done endoscopically or open. The procedure aims to release the affected compartment. To release the anterior and lateral leg compartments, an approximately 10cm longitudinal incision is made over the anterior lateral aspect of the leg between the tibial crest and the fibula. The anterior intermuscular septum between the compartments must be identified and the compartmental fascia can be released. A similar 10cm-incision on the medial aspect of the leg is utilized to access the superficial and deep posterior compartments. The superficial posterior compartment is easily identified and can be released directly but with cautious awareness of the neurovascular structures. To reach the deep compartment, undermine anteriorly and reach the posterior margin of the tibia, then detach the proximal soleus to visualize the deep posterior compartment and release it. In most instances, after adequate compartment release, skin closure is all that is needed as the surgeon does not want to compress the compartments again. The lower extremity can be placed in a soft dressing.
Post-operatively the patient can begin ice and elevation immediately. Active range of motion of the lower extremity can begin as tolerated. Weight bearing is allowed as tolerated. Typically, in 3-4 weeks post compartment release, the patient can begin to return to normal activity gradually.
The literature reports about a 4.5% to 11% complication rate associated with compartment release in the lower extremity. Most common complications noted are hemorrhage, infection, nerve entrapment, swelling, artery injury, hematoma, seroma, and deep vein thrombosis. Risk of recurrence of the exertional compartment syndrome is also possible, with a reported repeat rate of 3% to 12%.10
Campano et al2 completed a systemic review of the literature and found that 81% to 100% of the patients with chronic exertional compartment syndrome have pain relief after fasciotomies. The deep posterior compartment releases are less successful with a rate of 50% to 60%. Additionally, primary operative management of chronic exertional compartment syndrome was found to be successful in treating two-thirds of young athletic patients and 84% of patients were satisfied with their surgical outcomes at short- to mid-term follow up.
Popliteal Artery Entrapment
Popliteal artery entrapment syndrome has the most similar presentation to exertional compartment syndrome. In patients where chronic compartment syndrome is suspected, one must also examine and test for popliteal artery entrapment. Popliteal artery entrapment syndrome occurs when the popliteal artery becomes compressed by one of the calf muscles, typically the medial head of the gastrocnemius during exertion. This reduces blood flow to the leg and decreases oxygen perfusion to the muscles of the lower extremity. This leads to calf pain, cramping, and discomfort during exercise. The patient can also experience paresthesia and numbness. The symptoms are relieved by rest. The symptoms present remarkably similar to exertional chronic compartment syndrome. Testing for popliteal artery entrapment includes noninvasive vascular studies with exercise to evaluate the perfusion during exercise and with different leg positions. These patients are also typically evaluated by a vascular surgeon. An MRA (magnetic resonance angiogram) or CTA (computed tomography angiography) of the knee and tibia-fibula is typically ordered to evaluate the position of the popliteal artery relative to the other structures in the popliteal fossa. If these studies are inconclusive, a diagnostic angiogram can be obtained. If the patient is diagnosed with popliteal artery entrapment syndrome, treatment options include ceasing the activity which aggravates the symptoms or pursuing surgical intervention. Referral to vascular surgery or plastic surgery would be necessary at this step if surgical intervention for popliteal artery entrapment is needed. The goal of surgical intervention is to restore the abnormal relationship of the popliteal artery and the medial head of the gastrocnemius muscle and to decompress the four compartments of the leg. After surgery, vascular claudication is resolved rapidly, and the patient is typically able to return to activity. Post-operative MRA is typically performed around 4 months post-operatively to confirm adequate circulation.13,14
Conclusion
In conclusion, chronic exertional compartment syndrome and popliteal artery entrapment conditions are atypical causes of lower extremity pain in athletic patients. Both conditions should be ruled out in the work up of chronic lower extremity pain. After proper diagnosis and medical work up, most patients typically respond favorably with surgical intervention and aggressive post-operative physical therapy and rehabilitation.
Hayley Iosue, DPM, is a second-year fellow with the University Hospitals Advanced Foot and Ankle Fellowship. She completed her residency at Beth Israel Deaconess Medical Center in Boston, MA.
Joseph Albright, DPM, is a fellow with the University Hospitals Advanced Foot and Ankle Fellowship. He completed his residency at Aultman Alliance Community Hospital in Alliance, OH.
Mark Mendeszoon, DPM, is a senior partner at Precision Orthopaedic Specialties Inc. located in Chardon, OH. He is the director of University Hospitals Richmond Heights Medical Center Advanced Foot & Ankle Surgery. In addition, he is the owner of three Achilles Running Shops in Northeast Ohio and Erie, PA, as well as President of the Maple Leaf Track Club.
- Frontera W. Essentials of physical medicine and rehabilitation. Canada: Hanley and Belfus; 2002:256–261
- Campano D, Robaina JA, Kusnezov N, Dunn JC, Waterman BR. Surgical management for chronic exertional compartment syndrome of the leg: a systematic review of the literature. Arthroscopy. 2016;32(7):1478-86.
- Hislop M, Tierney P, Murray P, O’Brien M, Mahony N. Chronic exertional compartment syndrome: the controversial “fifth” compartment of the leg. Am J Sports Med. 2003;31(5):770-776.
- Brennan F, Kane S. Diagnosis, treatment options, and rehabilitation of chronic lower leg exertional compartment syndrome. Curr Sport Med Rep. 2003;2:247–250.
- Tucker AK. Chronic exertional compartment syndrome of the leg. Curr Rev Musculoskelet Med. 2010;3(1-4):32-7.
- Fraipont MJ, Adamson GJ. Chronic exertional compartment syndrome. J Am Acad Orthop Surg. 2003;11(4):268-276.
- Amendola A, Rorabeck CH, Vellet D, Vezina, Rutt B, Nott L. The use of magnetic resonance imaging in exertional compartment syndromes. Am J Sports Med. 1990;18(1):29–34.
- Balduini FC, Shenton DW, O’Connor KH, Heppenstall RB. Chronic exertional compartment syndrome: correlation of compartment pressure and muscle ischemia utilizing 31P-NMR spectroscopy. Clin Sports Med. 1993;12(1):151-165.
- Rajasekaran S, Kvinlaug K, Finnoff JT. Exertional leg pain in the athlete. PM&R. 2012;4(12):985-1000.
- Bong MR, Polatsch DB, Jazrawi LM, Rokito AS. Chronic exertional compartment syndrome: diagnosis and management. Bull Hosp Jt Dis. 2005;62(3-4):77-84.
- Pedowitz RA, Hargens AR, Mubarak SJ, Gershuni DH. Modified criteria for thediagnosis of chronic compartment syndrome of the leg. Am J Sports Med. 1990;18(1);35-40.
- Blackman PG, Simmons LR, Crossley KM. Treatment of chronic exertional anterior compartment syndrome with massage: a pilot study. Clin J Sport Med. 1998;8(1):14-17.
- Hicks CW, Black JH, Ratchford EV. Popliteal artery entrapment syndrome. Vasc Med. 2019;24(2):190-194.
- Gokkus K, Sagtas E, Bakalim T, Taskaya E, Aydin AT. Popliteal entrapment syndrome. A systematic review of the literature and case presentation. MLTJ. 2014;4(2):141.
- Sellers W, Obmann M, Nikam S, Song B, Mariner D. Popliteal artery entrapment syndrome presenting as acute limb ischemia in pregnancy. J Vasc Surg. 2017;3(4):232-235.