
Most people I have seen coming through my clinic with a shoulder issue have been told at some point that they have a rotator cuff tear. Or tendinitis of the rotator cuff. But when questioned further, they seldom know what’s torn or “damaged” just the rotator cuff…..
So what the hell is your rotator cuff?
Quick anatomy lesson:
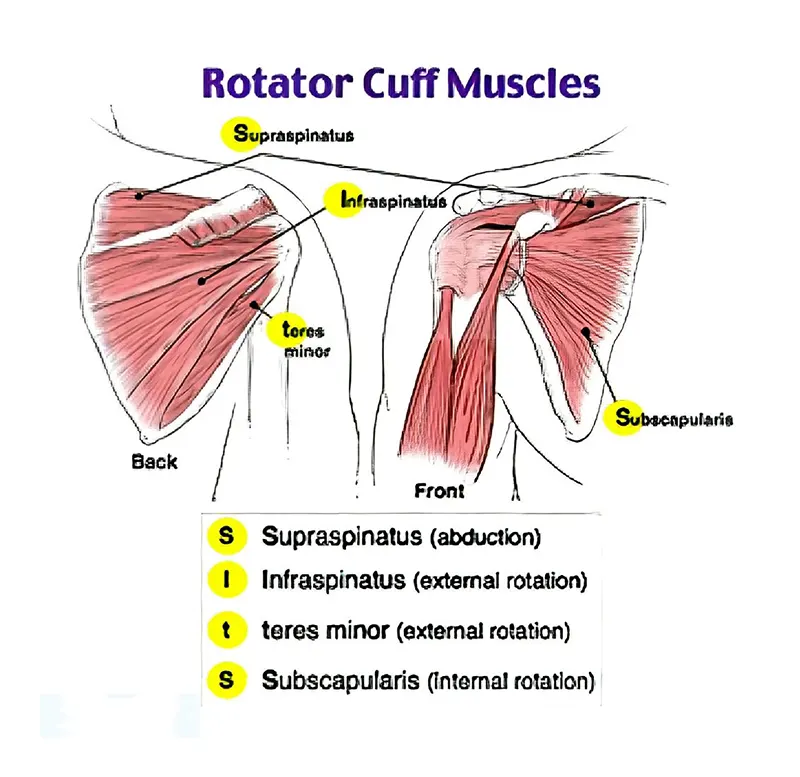
Your shoulder is a ball and socket joint much the same as your hip. The joint is much more shallow than the hip joint which is what makes it so susceptible to dislocation. The ball of the humerus is held in to the socket via the rotator cuff muscles. There are 4 rotator cuff muscles:
- Teres Minor
- Subscapularis
- Infraspinatus
- Supraspinatus
Teres minor:
Attaches on the outside border of the shoulder blade and to the top of the humerus. Its action is to work with the infraspinatus muscle to externally or outwardly rotate the arm.
Infraspinatus:
Attaches inside (infraspinous fossa) the scapula and also to the outside of the humerus. Assists with teres Minor in external rotation of the arm. Keeps the ball located in the socket of the shoulder.
Subscapularis:
Attaches on the front of the scapula (Subscapular fossa) and on to the outside top of the humerus. Its action is internal rotation of the shoulder (think arm wrestling muscle). It is assisted by the teres MAJOR muscle which is not technically a rotator cuff muscle, but is important.
Supraspinatus:
Attaches in the supraspinous fossa or in layman’s terms the very top of the shoulder blade. It inserts on the outside top of the humerus. Its action is to help in ABduction or lifting the arm away from the body sideways. The rest of the action is then taken over by the deltoid muscle.
As you can see, each of the muscles have a very different origin and action, however pretty much all attach in the same area of the upper arm. This is what creates the “cuff” that holds the ball of the humerus into the socket in the shoulder.
Rotator cuff Issues, causes and pitfalls of diagnosis
As I previously mentioned, most people who come in with with shoulder pain have more than likely at some stage been told that they have a torn rotator cuff. Now, from our little anatomy lesson we can see that there’s a problem in that, what exactly did they tear? The rotator cuff is not just one single thing. Its a group of muscles all with different tendinous attachments into a similar point on the arm.
There are 2 types of tear, a full tear and partial tear. A full tear is a proper rupture of the tendon and tends to require surgical reattachment. A partial tear is when small micro tears appear in the tendons as a result of continual use. People who partake in over head activities or who need to go through full rotations of the arm tend to have partial tears in the rotator cuff.
Tendinitis and Tendinosis are also common diagnosis for rotator cuff injuries. This is when the tendon becomes inflamed from repetitive use. Chronic tendinitis is known as tendinosis. A common reason tendons become inflamed, and can lead to micro tears in is that the shoulder is compressed. This reduces the space between the acromion and the top of the shoulder blade meets the collarbone or clavicle. This is often called a subacromial impingement where the bone effectively pinches the tendon every time the arm i raised or rotated. Common practice in this case is to give generic rotation exercises, or steroid injections in to the area. The success rate for this is in fact quite slim. Many often opt for a surgical option called an acromioplasty which shaves down the bone and in theory creates space for movement of the shoulder. Again, success for this surgery is minimal, and in fact I personally have seen more than one instance where its made the injury worse!
Conventional treatment and its pitfalls
So what’s the problem with conventional treatment? The problem is it doesn’t address the underlying issue. The shoulder becomes compressed because muscles surrounding the shoulder become tight and keep it sucked in there. And this isn’t just isolated to the rotator cuff muscles. Any muscle that has any dealings with how the shoulder moves in any direction can impact how the rotator cuff works. Impact injuries can also cause shoulders to compress and muscles around it become short and tight as a protective mechanism.
Let’s take the pec minor, seen below in red, for example:
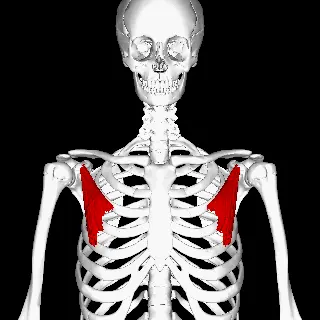
This attaches to the front of the ribs and into the corocoid process of the scapula. It rotates the shoulder forward bringing the shoulder blade up with it. When we do that, instantaneously we reduce the space available for the arm to move. If you are in that state on a daily basis you will start getting impingement in at the acromion process leading to tendonitis. So most people would work in on the rotator cuff and try rehab that injury, whereas in fact, it’s the pec minor they should really be concentrating on.
Try it for yourself. Raise your arm out to the side up to your head. Now roll your shoulder forward and try it again. See the difference?
Here’s something else I want you to try. Raise your shoulder out to the side. See what range of motion you have. Now tilt that shoulder down to the side. Try and raise your arm again. Notice a difference? So what scenario might this happen? Think about a sprained foot. You compensate by leaning to the other side, away from the sprained foot. You now have a tilted shoulder to one side, reducing the space for the shoulder to move. So again, whats the more important thing to treat here? The sprained ankle, not the shoulder.
Another thing to highlight is that in fact there is very little correlation between micro or partial tears of a tendon and shoulder pain. All too often it is attributed to someone’s pain and it can lead down the road of expensive and unnecessary surgery.
So what can be done? First off the best thing you can do is stop or avoid injections into the painful area, as well as doing countless shoulder rotations to try and fix the issue. THE BEST course of action is to get yourself assess properly and try and get to the proper bottom of the issue. AND PLEASE avoid surgery if at all possible!



